E. coli Risk Profile

Escherichia coli are in the family Enterobacteriaceae, gram negative, rod shaped, non-spore forming, and motile or non-motile. Escherichia coli is a predominant enteric species in the human gut and, it is a part of the normal intestinal flora, which provides many health benefits to the host; i.e., they prevent the colonization of the gut by harmful pathogens. On the other hand, certain specific groups of E. coli, are referred to as enterovirulent E. coli, diarrheagenic E. coli, or more commonly, pathogenic E. coli that can cause severe diarrheal diseases in humans. At present, there are six recognized pathogenic groups in the E. coli family, that are enterotoxigenic E. coli (ETEC), enteropathogenic E. coli (EPEC), enterohemorrhagic E. coli (EHEC), enteroinvasive E. coli (EIEC), enteroaggregative E. coli (EAEC), and diffusely adherent E. coli (DAEC). EHEC is the major foodborne outbreaks contributor worldwide. The first four groups are well known to be transmitted via contaminated food or water. Pathogenic E. coli are generally grouped based on their virulence properties or factors that they carry, but certain groups can share similar virulence traits such as both EPEC and EHEC produce intimin protein, which allows the pathogen to attach to intestinal cells. Furthermore, many of the virulence genes carried by these pathogenic E. coli groups reside on mobile genetic elements and can be transferred.
Growth Factors
Temperature:
Minimum – 6°C Maximum – 50°C (Optimum
35°C – 40°C)
pH:
Minimum
– 4 Maximum – 10 (Optimum
6 – 7)
Water Activity (aW):
Minimum
– 0.95 Maximum – - (Optimum
0.995)
Water Phase Salt:
Maximum
– 6.5%
Enteropathogenic Escherichia coli (EPEC)

EPEC are gram-negative,
rod-shaped bacteria, which are characterized by the presence of the locus for
enterocyte effacement (LEE) pathogenicity island, which carries multiple
virulence factors, including the eae gene that encodes for intimin and,
together with the tir gene (intimin receptor), allows intimate adherence of
EPEC to intestinal epithelial cells. In the 1940s and 1950s, EPEC was a
frequent cause of infantile diarrhea in the US, but it is less important in
developed countries as of now. However, EPEC continues to be a common cause of
diarrhea in developing countries, especially in children less than two years
old.
Sources
Source(s) and prevalence of EPEC are controversial, as foodborne
outbreaks are sporadic. Foods implicated in past EPEC outbreaks have included
raw beef and chicken, but any food exposed to fecal contamination is strongly
suspect. There are reported cases that were traced back to mayonnaise, lettuce,
and pickles.
Disease

The disease usually
associated with EPEC is infantile diarrhea.
Mortality:
Mortality rates from 25%
to 50% have been reported in the past, but, better treatment and medical
facilities have greatly reduced mortality in the developed countries, however,
the number of deaths is still positive.
Infective dose:
EPEC is highly infective
in infants, where the dose is usually very low, but adults are not as
susceptible as infants. Volunteer feeding studies have established that 10
million to 10 billion cells are required to cause diarrhea in adults, provided
that gastric acid first has been neutralized by bicarbonate.
Onset:
The onset of diarrhea is
often rapid, occurring as soon as 4 hours post-ingestion of EPEC.
Complications:
Diarrhea may be mild,
but the infection occasionally can be severe, where fluid and electrolyte
imbalance may require to be corrected, to prevent dehydration.
Symptoms:
Profuse, watery
diarrhea; vomiting; and low-grade fever.
Duration:
Diarrhea occasionally is
protracted, lasting from 21 to 120 days.
Route of entry:
Oral.
Pathway:
After ingestion, EPEC
adheres to the intestinal mucosa and causes extensive disarrangement of the
digestive-absorptive enzyme system, which results in malabsorption of
nutrients.
Frequency

EPEC Foodborne outbreaks
are irregular in nature and incidence varies around the world depending on the
individual country’s health system, where countries with poor sanitation
practices have the most frequent outbreaks. Nonetheless, frequent records of
out brakes occur in day-care centers and pediatric wards.
Diagnosis
Culture of stools from infected people for E. coli and testing
the isolates for the ability to cause attachment and effacing (A/E) lesions on
tissue culture cells.
PCR assays are used to test the isolates for LEE genes, but
Enterohemorrhagic E. coli (EHEC) also carries LEE, thus isolates have to be
further tested for Shiga toxins (Stx). EPEC is distinguished from EHEC by the
presence of LEE and the absence of Stx.
Target Populations
The most vulnerable to the EPEC infections are infants;
especially those who are being bottle fed, because poor quality water used to
rehydrate infant formulae in underdeveloped countries may be the source of EPEC
in bottle-fed infants.
Food Analysis
The presence of EPEC in foods can be distinguished by plating
culture enrichment of food samples onto media that are selective and
differential for E. coli. Then test the isolates for EPEC traits by tissue
culture or PCR. Finally, Shiga toxins (Stx) assays are essential to distinguish
EHEC from EPEC, where EPEC is characterized by the presence of LEE and the
absence of Stx.
Enterotoxigenic Escherichia coli (ETEC)

Enterotoxigenic Escherichia coli (ETEC) are highly motile, Gram-negative, rod-shaped bacteria, which are characterized by the production of several virulence factors, including several colonization-factor antigens as well as heat-labile (LT) toxin and heat-stable (ST) toxins.
Sources
Most ETEC outbreaks are linked to the consumption of
contaminated food or water. ETEC is often found in feces of asymptomatic
carriers, and humans appear to be the most likely source of ETEC. In 1975, a
large outbreak affecting 2,000 people was traced to sewage-contaminated water
at a national park. Contaminated well water in Japan and water supplies aboard
cruise ships also have been implicated in ETEC outbreaks. Foodborne outbreaks
of ETEC have occurred in restaurants and at various catered functions. Examples
of implicated foods include Brie cheese, curried turkey, mayonnaise, crabmeat,
deli food, and salads. In most of these cases, foods became contaminated with
ETEC via infected food handlers or through the use of contaminated water during
preparation. ETEC infection does not appear to be transmitted by
person-to-person contact, but some hospital infections have occurred and
probably were caused by unsanitary conditions.
Disease
ETEC causes gastroenteritis in humans and is best known as the
causative agent of travelers’ diarrhea, and an important cause of diarrhea in
infants, in underdeveloped countries.
Mortality:
The World Health
Organization attributes 380,000 deaths (worldwide) to ETEC, mostly among
children, each year.
Infective dose:

Children can be affected by a smaller dose, but according to the volunteer feeding studies; a high dose ranging from 10 million to 10 billion ETEC cells, may be required to cause an infection in adults.
Onset:
The range is around 8 to
44 hours, but usually after 26 hours of ingestion of contaminant.
Complications:
Infection from ETEC is
usually self-limiting, mild, and brief, but certain severe stains may last
longer and resemble cholera, with up to five or more daily passages of
liquefied stools that result in severe dehydration. Antibiotic treatment is not
usually recommended for ETEC infections, but effective in reducing the duration
and severity of illness. Appropriate electrolyte replacement therapy may be
necessary for infants and elderly or susceptible patients.
Symptoms:
Characterized by the
sudden onset of watery diarrhea without blood or mucus, which is rarely
accompanied by high fever or vomiting. Further symptoms include abdominal
cramps, low-grade fever, nausea, and malaise.
Duration of symptoms:
Most cases last a few
days, but severe forms can last up to 19 days.
Route of entry:
Oral.
Pathway:
ETEC colonizes in the
small intestine after ingestion and releases toxins that induce fluid
secretion.
Frequency
ETEC outbreaks are infections that are a more common occurrence
among international travelers, but it is rare in the United States. ETEC
infections are more prevalent in the warmer, wet months and endemic to many
developing countries and areas in tropics with poor hygiene standards.
Diagnosis

Large numbers of ETEC cells are excreted in feces during the acute phase of infection, but generic E. coli cells are also present in large quantities on the bowels. Thus, ETEC strains can be differentiated from other E. coli by in vitro immunochemical assays, tissue culture, or gene probes and PCR assays specific for LT and ST toxin genes. Antibody test kits that detect these toxins are commercially available in the market.
Target Populations
Infants and travelers to underdeveloped countries are most at
risk of ETEC infection. Immunocompromised people are more likely than others to
suffer severe, even life-threatening causes.
Food Analysis
The presence of ETEC in foods can be distinguished by plating
culture enrichment of food samples onto media that are selective and
differential for E. coli. Then test the isolates for LT and ST toxins, using
PCR or commercial kits with specific antibodies for the toxins. ETEC analyses
are not performed usually because of its high infectious dosage unless generic
E. coli levels are very high.
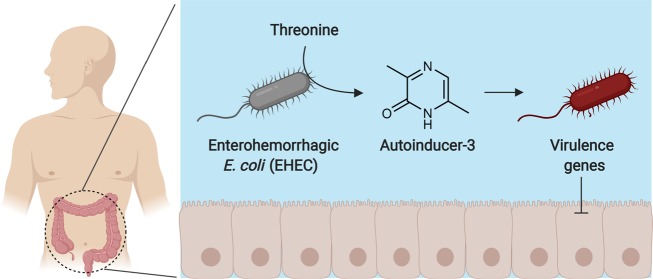
Enterohemorrhagic Escherichia coli (EHEC)
Toxin-producing Shiga-toxigenic Escherichia coli (STEC) are
Gram-negative, rod-shaped bacteria like generic E. coli, but are categorized
differently due to the production of Shiga toxins (Stx). There are 200 to 400
STEC serotypes that are referenced, many of which have not been implicated in
human illness. However, a subset of STEC called enterohemorrhagic Escherichia
coli (EHEC) causes serious infection by the prototypic EHEC strain, which is
the well-known serotype O157:H7. Although O157:H7 is currently the predominant
strain and accounts for ~75% of the EHEC infections worldwide, other non-O157
EHEC serotypes are emerging as a cause of foodborne illnesses.
EHEC is characterized by the production of Stx, including Stx1
and/or Stx2, and the presence of LEE. There are also several other putative
virulence factors, including enterohemolysin, but the role of these factors in
pathogenesis remains undetermined.
Sources

Raw or undercooked ground beef and beef products are the vehicles most often implicated in O157:H7 outbreaks. Earlier outbreaks also implicated the consumption of raw milk. O157:H7 can develop acid tolerance, as evidenced by infections in which acid foods. Further, there are several outbreaks that were traced back to unpasteurized juices, lettuce, salads, various types of sprouts, and spinach. EHEC infections caused due to various water sources including potable, well, and recreational water, which was in contact with animals at farms or petting zoos, besides person-to-person transmission of the infection is well documented.
Disease
EHEC infection can be life threatening from the less
serious form of the infection, which can range from no symptoms to diarrhea
that starts out watery, then turns bloody.
Mortality:
Patients whose infection
progresses to HUS (Hemolytic–uremic syndrome) have a mortality rate of 3% to 5%.
Infective dose:
The infective dose of
EHEC O157:H7 is estimated to be very low, in the range of 10 to 100 cells, but
the infective dose of other EHEC serotypes is suspected to be slightly higher.
Onset:
Symptoms usually begin 3
to 4 days after exposure, but the time may range from 1 to 9 days.
Complications:
Infections from EHEC can
be progress to severe complications from asymptomatic-to-mild diarrhea. The
acute symptoms are characterized by severe abdominal cramps and bloody diarrhea
called hemorrhagic colitis (HC), and 3% to 7% of HC cases may progress to such
life-threatening complications as HUS or thrombotic thrombocytopenic purpura
(TTP). These conditions are most often associated with O157:H7, which also can
occur with other EHEC serotypes. Survivors occasionally develop permanent
disabilities, such as renal insufficiency and neurological deficits. Antibiotic
therapy for EHEC infection has had mixed results and, in some instances, seems
to increase the patient’s risk of HUS. One speculation is that antibiotics lyse
EHEC cells, releasing more Stx into the host.
Symptoms:
Hemorrhagic colitis is
characterized by severe cramping (abdominal pain), nausea or vomiting, and
diarrhea that initially is watery, but becomes grossly bloody. Diarrhea may be
extreme in certain cases, appearing to consist entirely of blood and occurring
every 15 to 30 minutes, where fever is typically low-grade or absent.
Duration:
In uncomplicated cases,
the duration of symptoms is 2 to 9 days, with an average of 8 days.
Route of entry:
Oral.
Pathway:
After ingestion, EHEC
moves through the gastrointestinal tract and attaches to intestinal epithelial
cells via LEE-encoded factors. The start the production of Stx that is
internalized, activated and can pass into the bloodstream to become systemic.
Frequency
Ground beef and beef products continue to be implicated in most
infections; however, contaminated produce increasingly has been implicated as a
vehicle. STEC non-O157 attributed to foodborne infections are estimated to be
112,752 per year. The EHEC infections further attribute to 63,000 yearly in the
US, according to a report by the Centers for Disease Control and Prevention
(CDC).
There are about 63,000 cases of EHEC infections in the United
States annually, where ground beef and beef products continue to be implicated
in most infections. But contaminated fresh produce has been a rising concern in
recent incidents. However, the STEC non-O157 infections account for 112,752
cases per year according to the CDC.
Diagnosis
Bloody diarrhea samples of patients are plated onto sorbitol MacConkey medium to screen for sorbitol non-fermenting isolates, which are then typed serologically using antibodies to the O157 and the H7 antigens. Because EHEC O157:H7 does not ferment the sugar sorbitol like generic E. coli However, clinical samples are simultaneously tested for the presence of Stx using commercially-available antibody kits now, and then serotyped and identify the STEC strains. PCR assays specific for Stx genes are also available, that may be used for screening clinical samples.
Target Populations
Young children and the elderly population are more susceptible
and at higher risk for the infection to develop into more severe complications,
but every human is believed to be susceptible to hemorrhagic colitis.
Immunocompromised people are also at high risks, such as some chronic diseases
or AIDS, and people on immunosuppressive medications; for example, some drugs
used for arthritis and cancer chemotherapy.
Food Analysis
The generic E.coli testing procedures are initially conducted prior to serological testing for the O157 and H7 antigens and also for the presence of Stx genes by PCR. Presence of EHEC O157:H7 in foods can be determined by plating culture enrichment of food samples onto selective and differential media. O157:H7 does not ferment sorbitol and negative with the MUG assay. Molecular assays can specifically detect O157:H7 strains using unique mutational markers. However, the detection of non-O157:H7 EHEC, is more complex due to the lack of unique traits. For non-O157 EHEC, food enrichment is first screened for Shiga toxin using an antibody assay or for Stx genes by PCR. The process is time-consuming and labor-intensive, which may require screening hundreds of isolates.
Reference:
FDA Bad Bug Book, Foodborne Pathogenic Microorganisms and Natural Toxins. Second Edition. 2013
Preventive Controls for Human Foods. 2016
www.cdc.gov
No comments:
Post a Comment